Monocyte Cells
https://en.wikipedia.org/wiki/Monocyte
Monocytes influence adaptive immune responses and exert tissue repair functions. Monocytes are mechanically active cells and migrate from blood to an inflammatory site to perform their functions. In general, monocytes and their macrophage and dendritic cell progeny serve three main functions in the immune system. These are phagocytosis, antigen presentation, and cytokine production. Phagocytosis is the process of uptake of microbes and particles followed by digestion and destruction of this material. Monocytes can perform phagocytosis using intermediary proteins such as antibodies or complement that coat the pathogen, as well as by binding to the microbe directly via pattern recognition receptors that recognize pathogens.
Monocytes are also capable of killing infected host cells via antibody-dependent cell-mediated cytotoxicity. Vacuolization may be present in a cell that has recently phagocytized foreign matter.
https://haematologica.org/article/view/5308
Monoblasts are normally found in bone marrow and do not appear in the normal peripheral blood.
Monoblast are of hemopoietic stem cell progression:
monoblast -> promonocyte -> monocyte-> macrophage/dendritic cell.
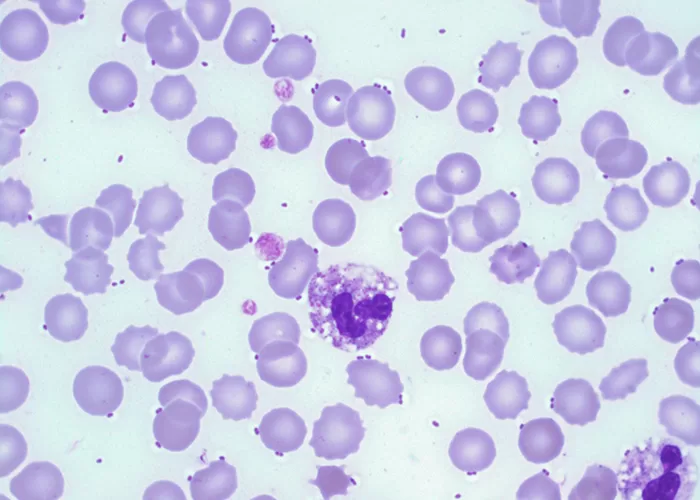
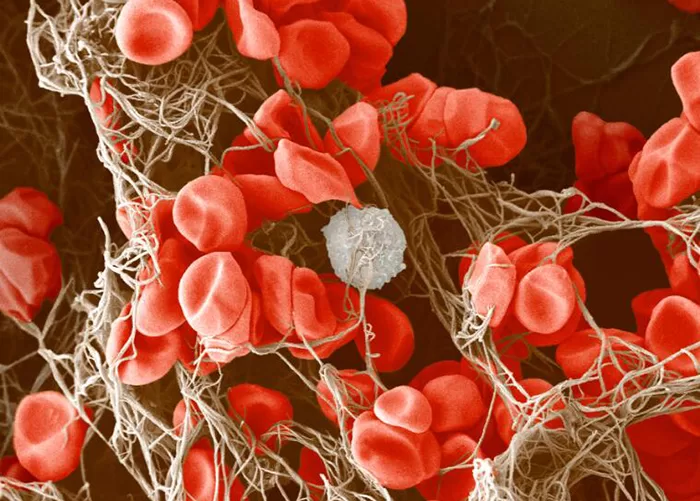
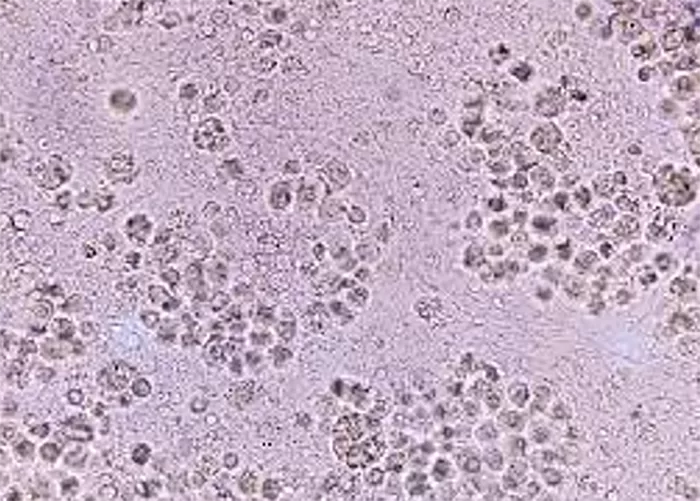
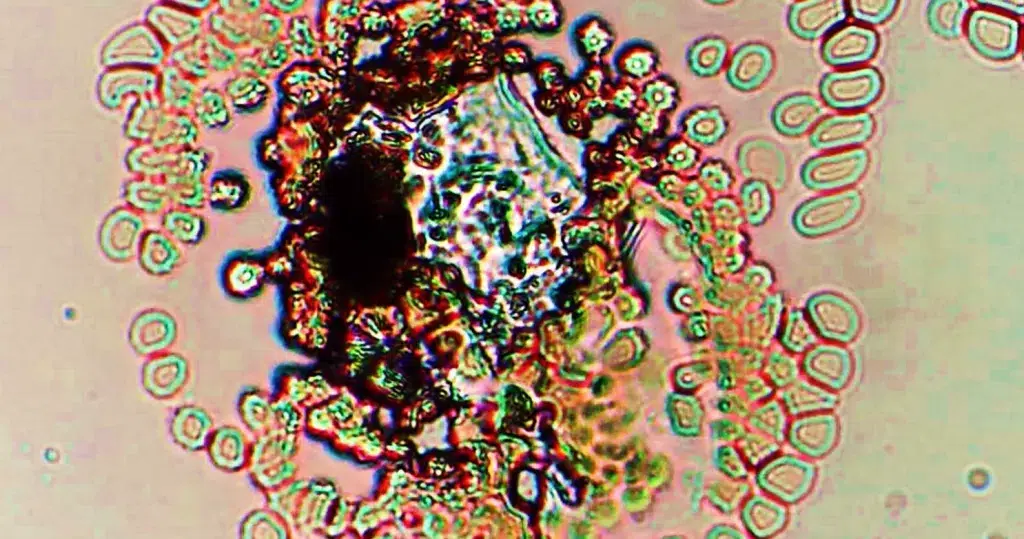
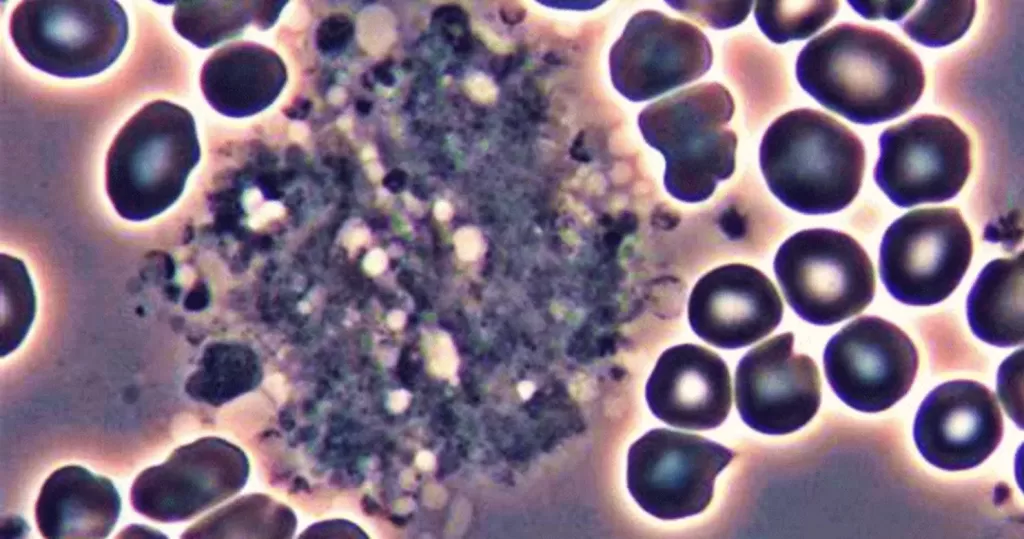
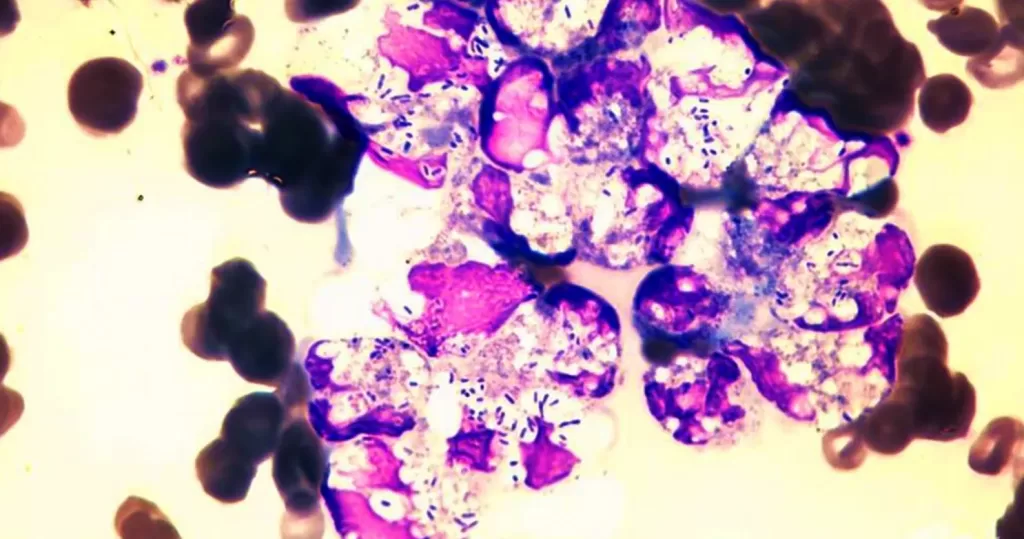
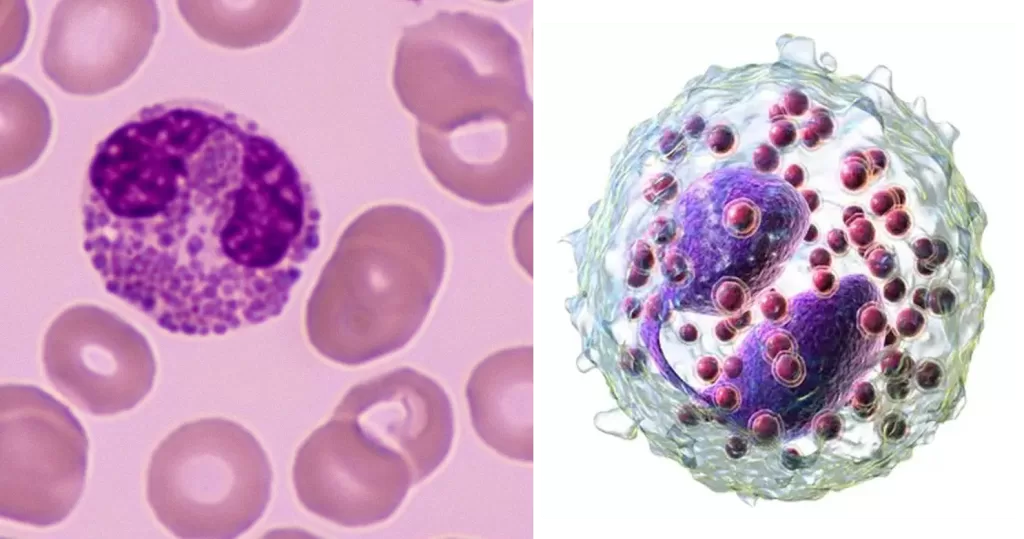
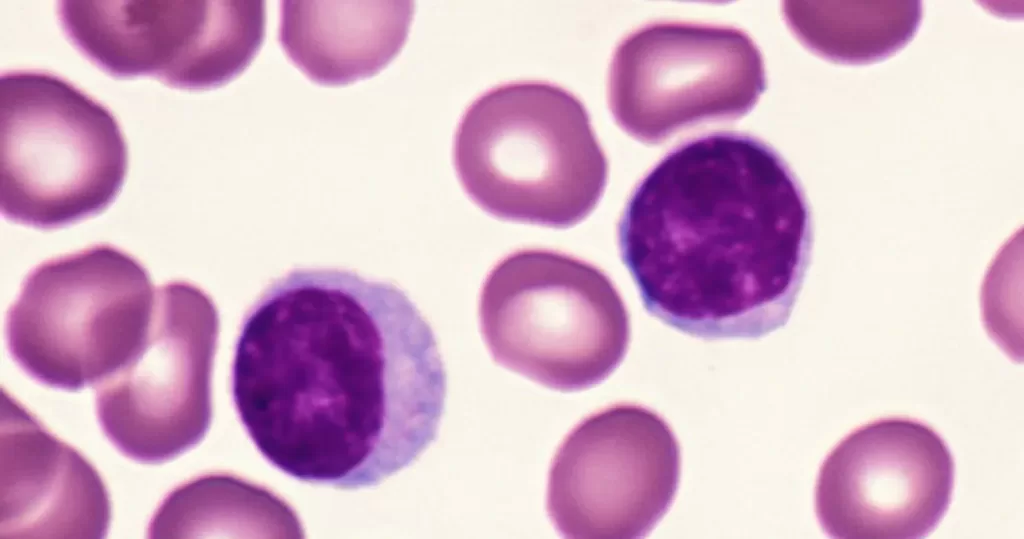
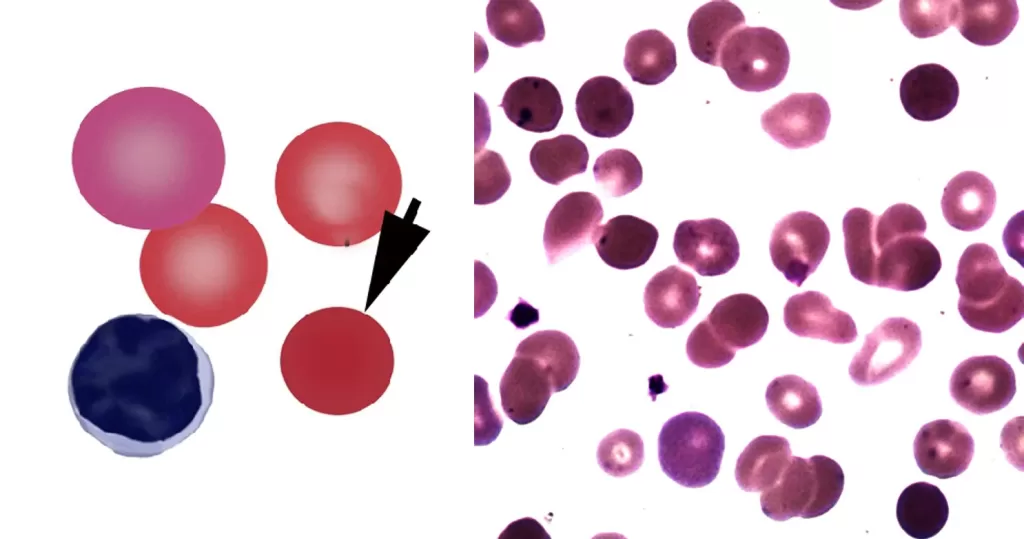
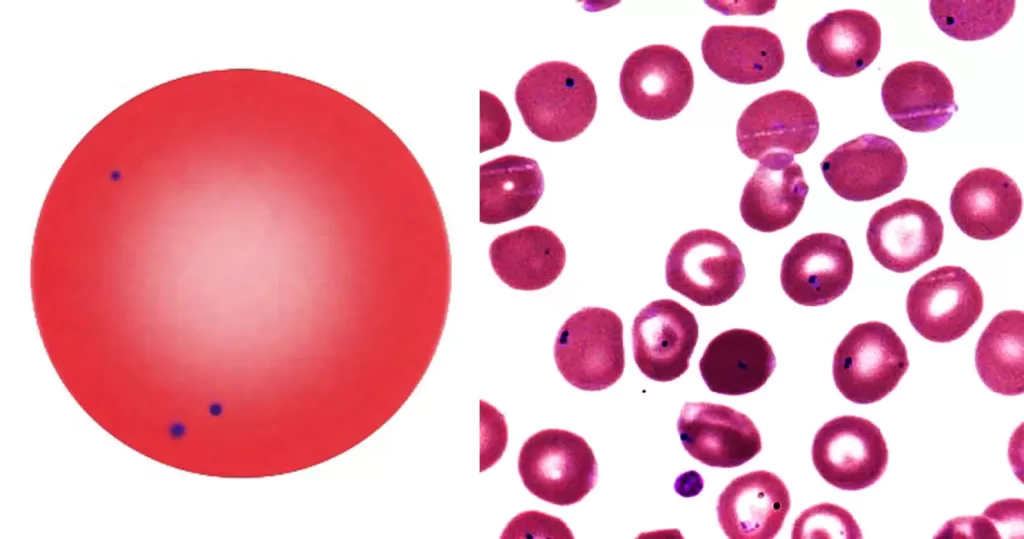
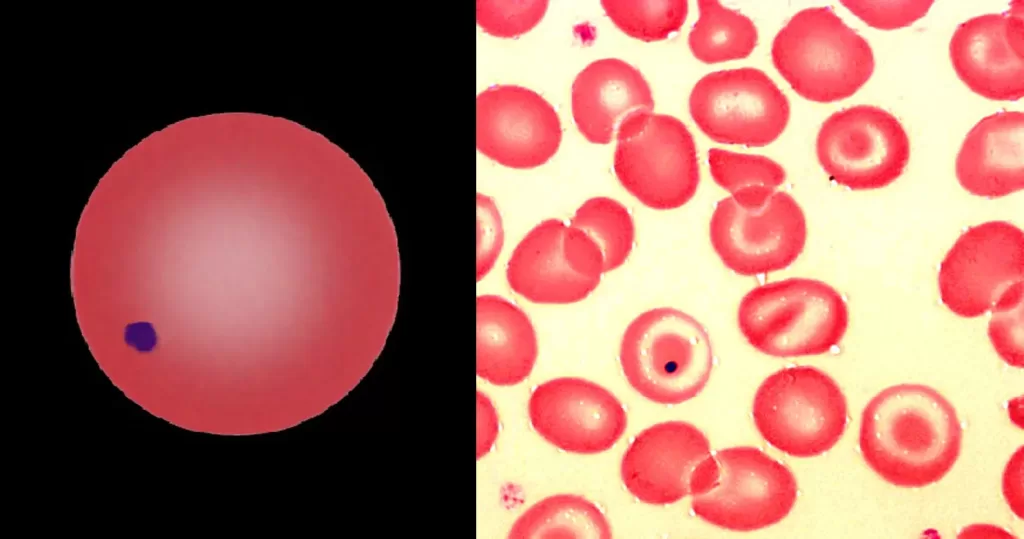
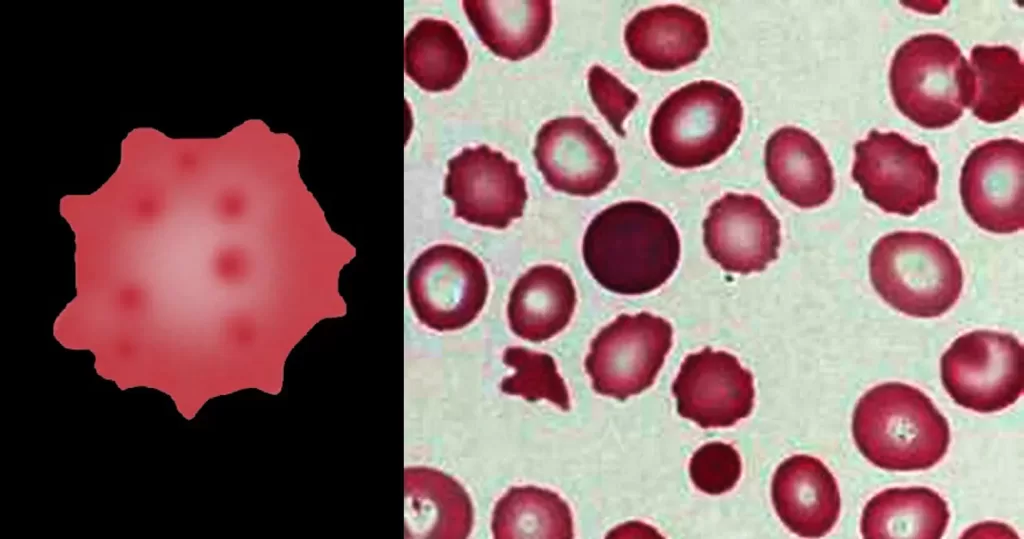
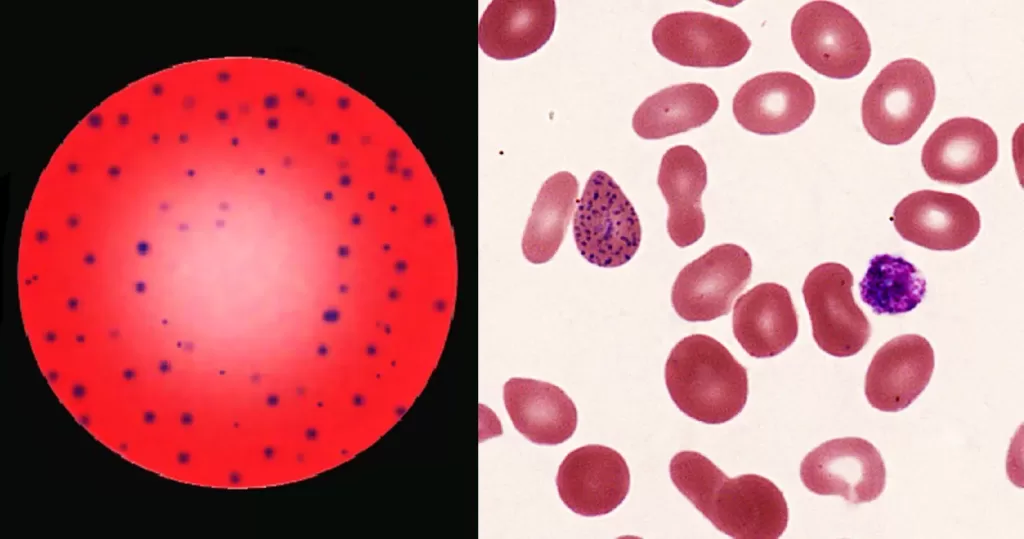
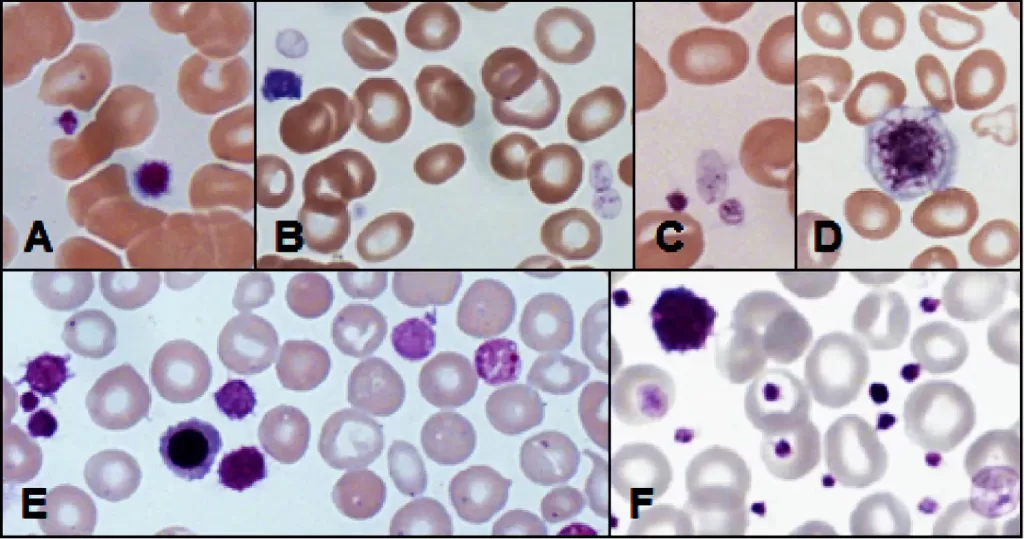
Active monocyte. Notice the whites dots, which are toxins or debris the monocyte consumed from entities it suctions. The nucleus can have a “U” shape appearance.
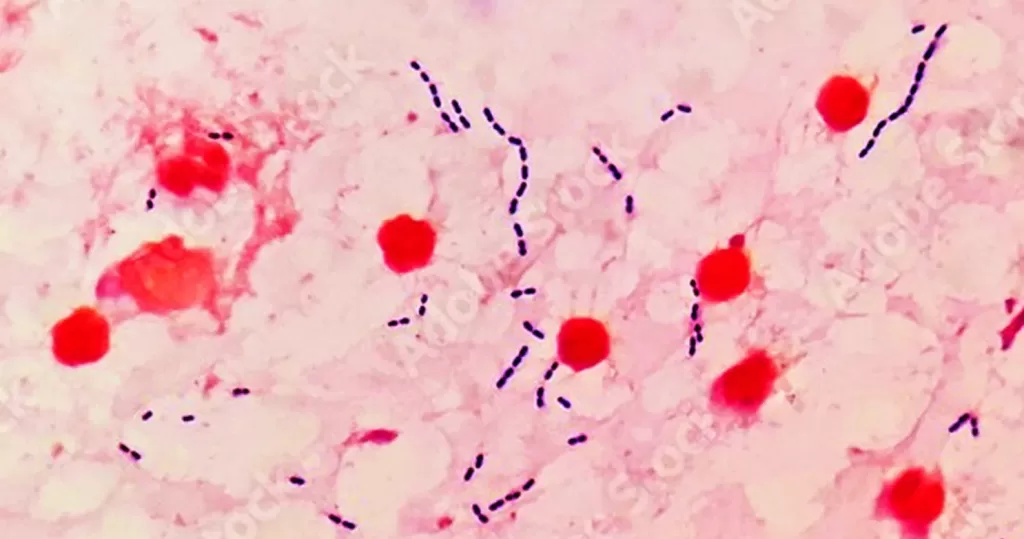
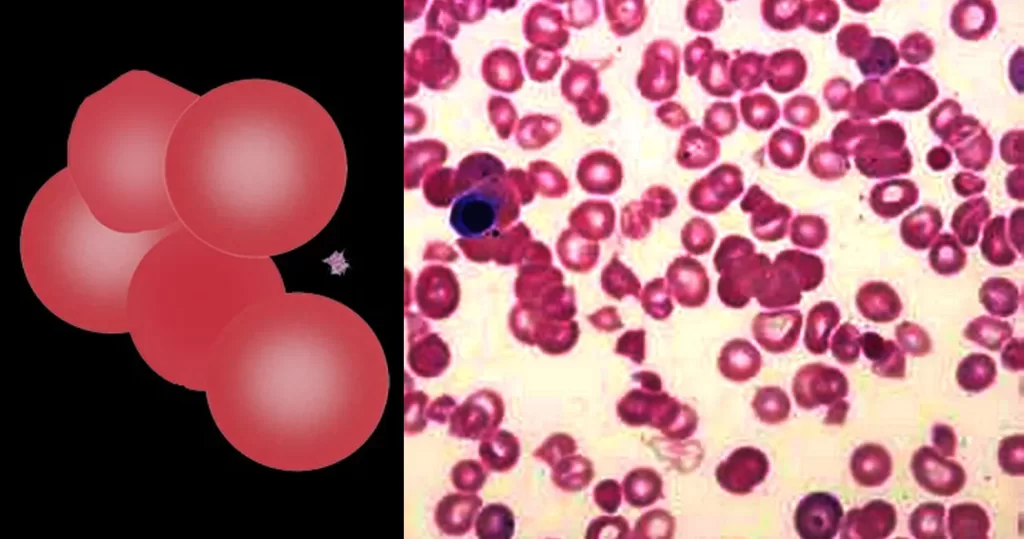
Acute Monocyte Leukemia.
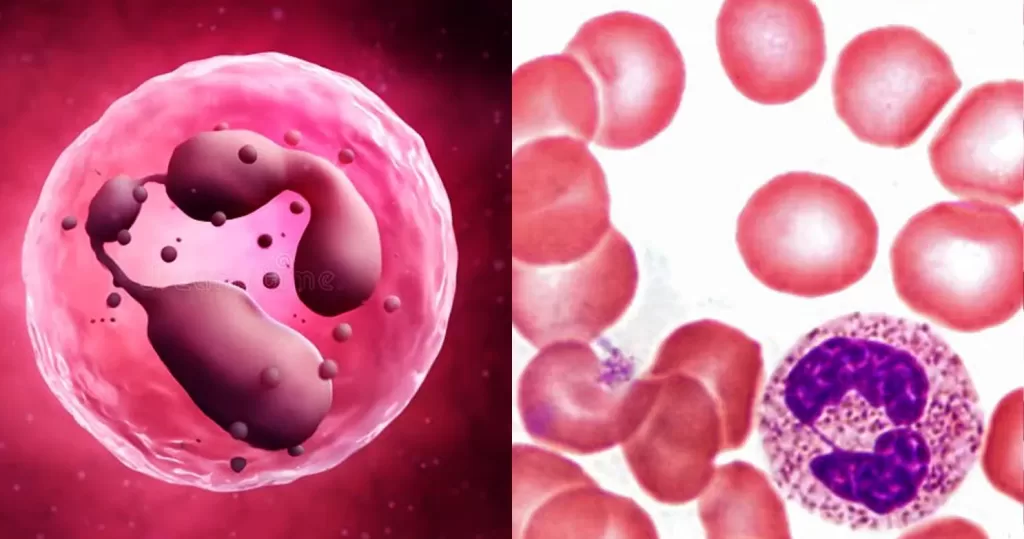
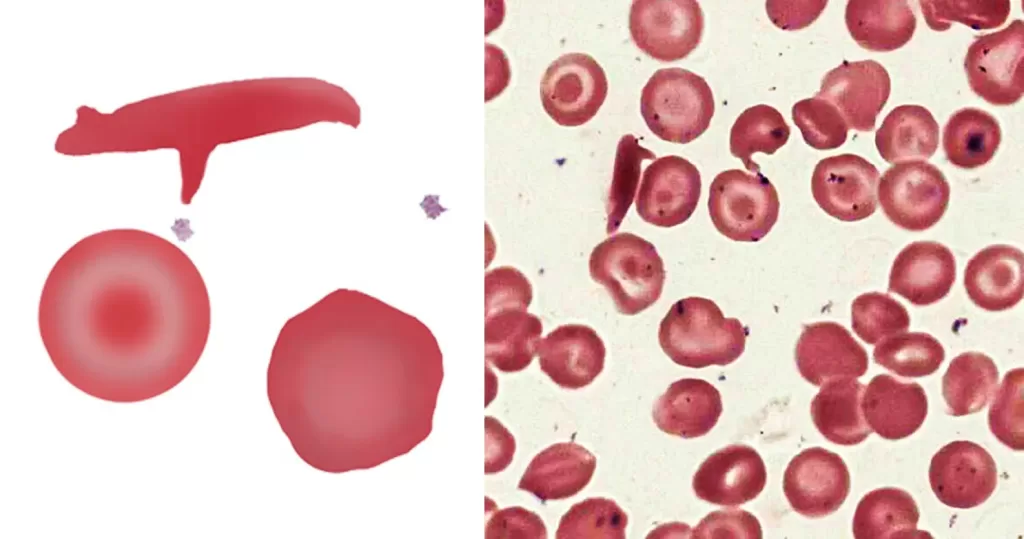
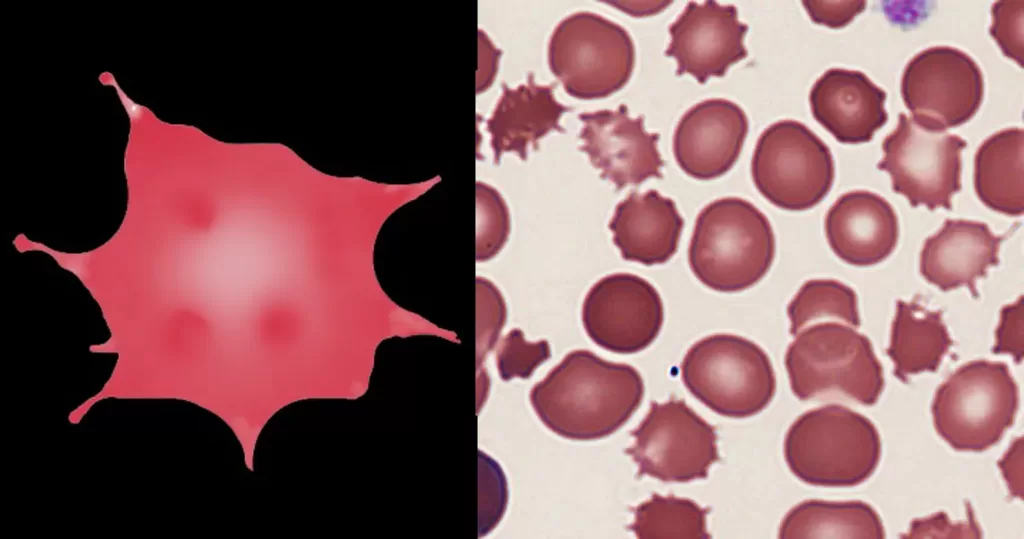
Toxic Neutrophil – toxins that it has acquired have melted the nuclei.
Monocytosis (high levels). Often occurs during chronic inflammation.
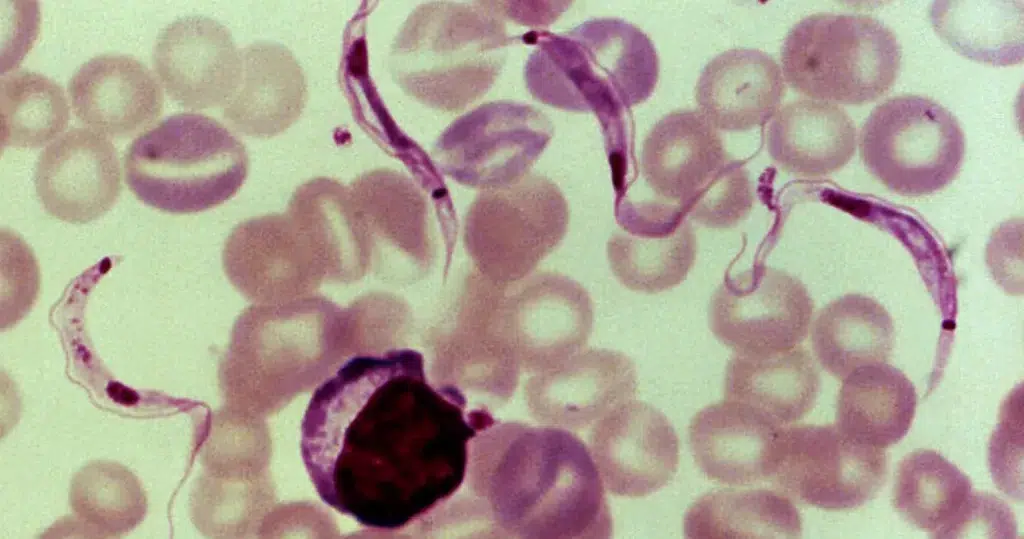
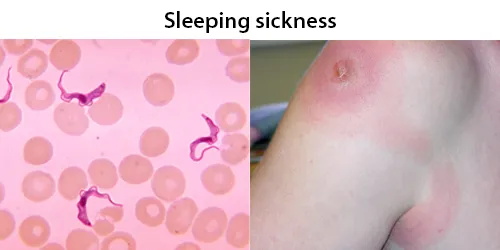
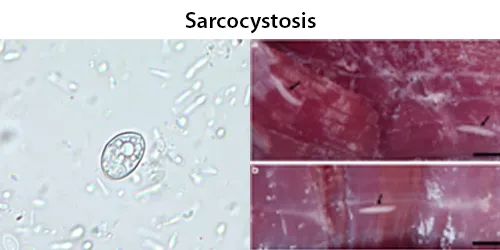
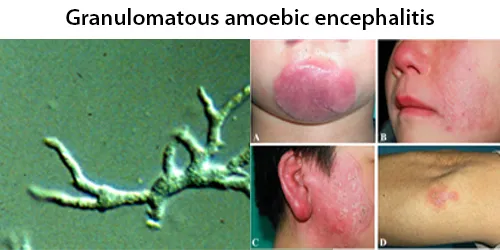
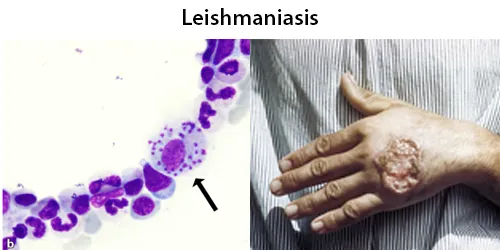
- Infections: tuberculosis, brucellosis, listeriosis, subacute bacterial endocarditis, syphilis, and other viral infections and many protozoal and rickettsial infections (e.g. kala azar, malaria, Rocky Mountain spotted fever).
- Blood and immune causes: chronic neutropenia and myeloproliferative disorders. Autoimmune diseases and vasculitis: systemic lupus erythematosus, rheumatoid arthritis and inflammatory bowel disease.
- Malignancies: Hodgkin’s disease and certain leukaemias, such as chronic myelomonocytic leukaemia (CMML) and monocytic leukemia.
- Recovery phase of neutropenia or an acute infection.
- Obesity.
- Miscellaneous causes: sarcoidosis, drug overdose, lipid storage disease and ZNFX1 deficiency.
Monocytopenia (low levels). Causes include: acute infections, stress, treatment with glucocorticoids, aplastic anemia, hairy cell leukemia, acute myeloid leukemia, treatment with myelotoxic drugs, intestinal resection, and genetic syndromes, as for example MonoMAC syndrome.
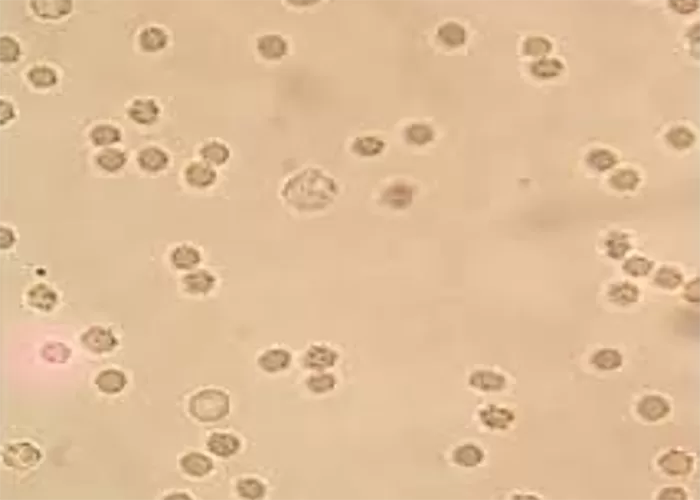
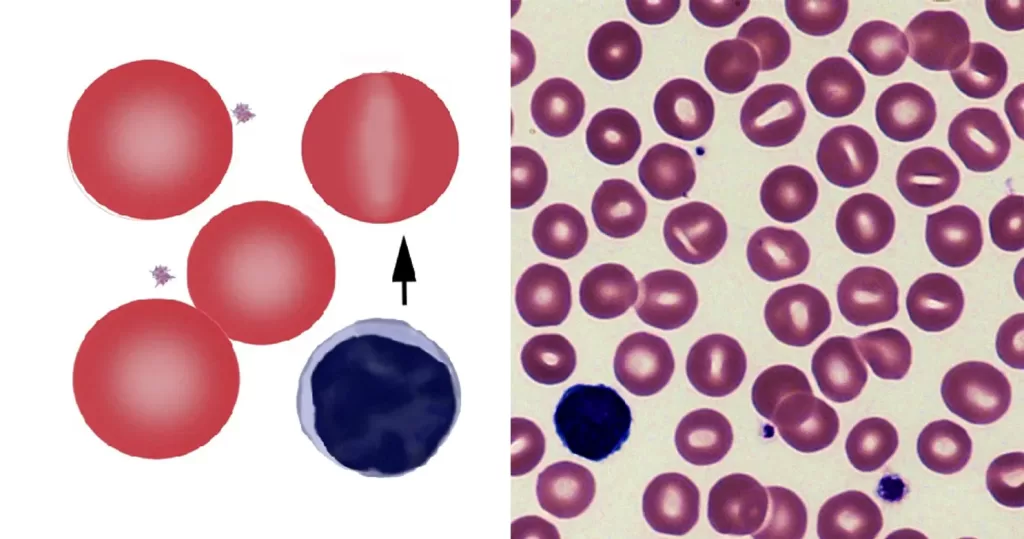
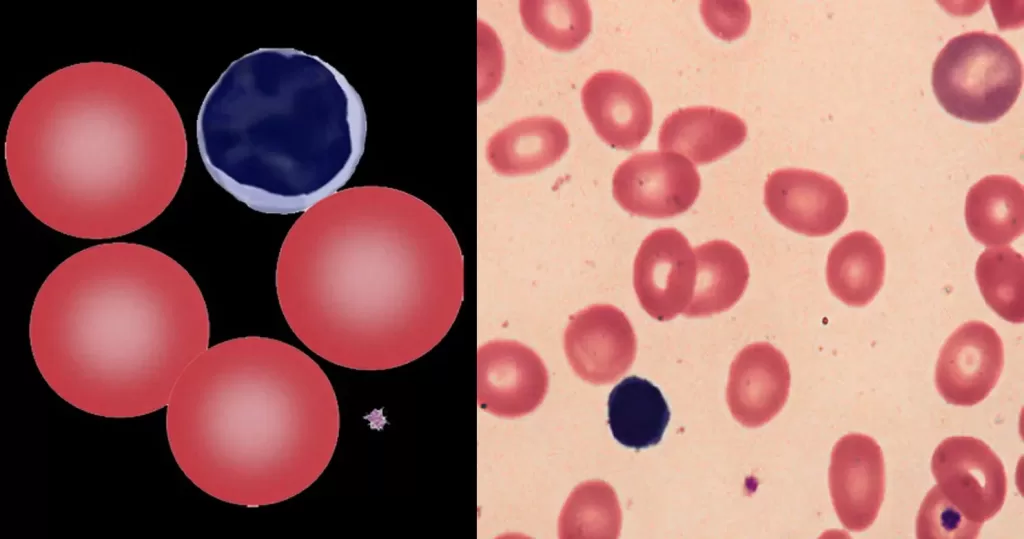
Unstained monocytes (3 total) with adjoining neutrophils (2 total).
Indication of active and healthy immune response.
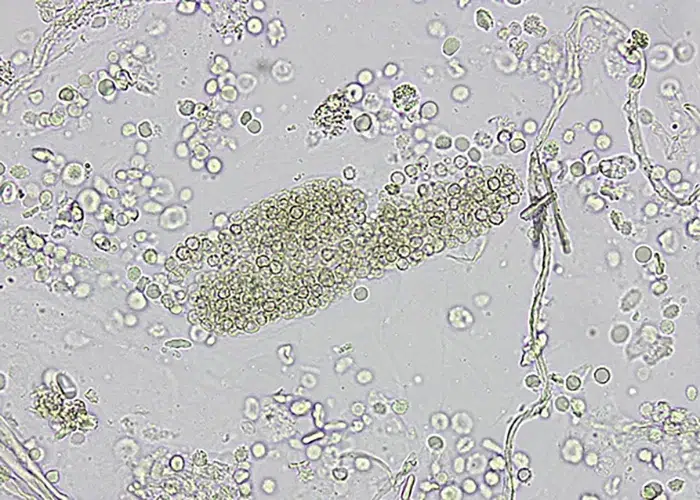
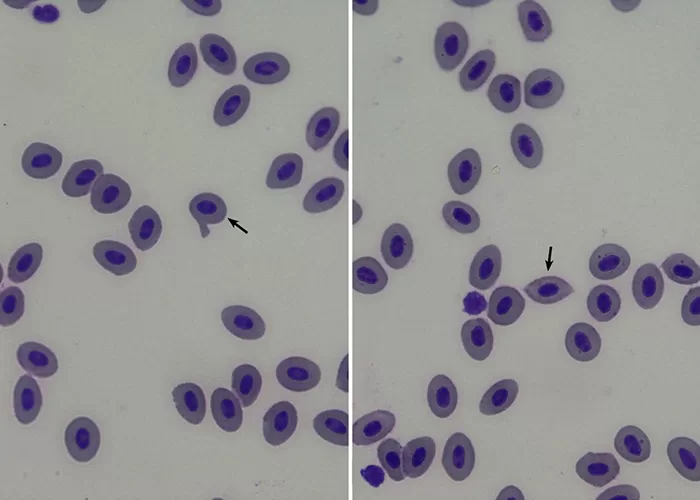
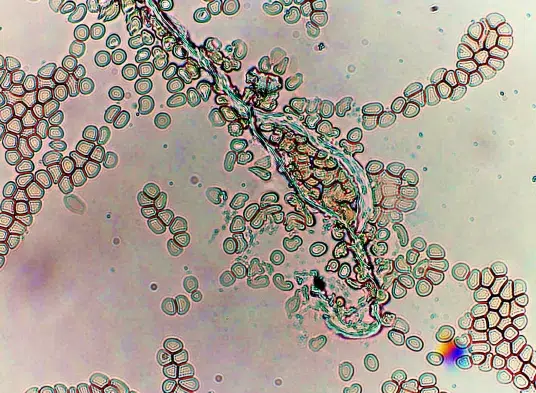
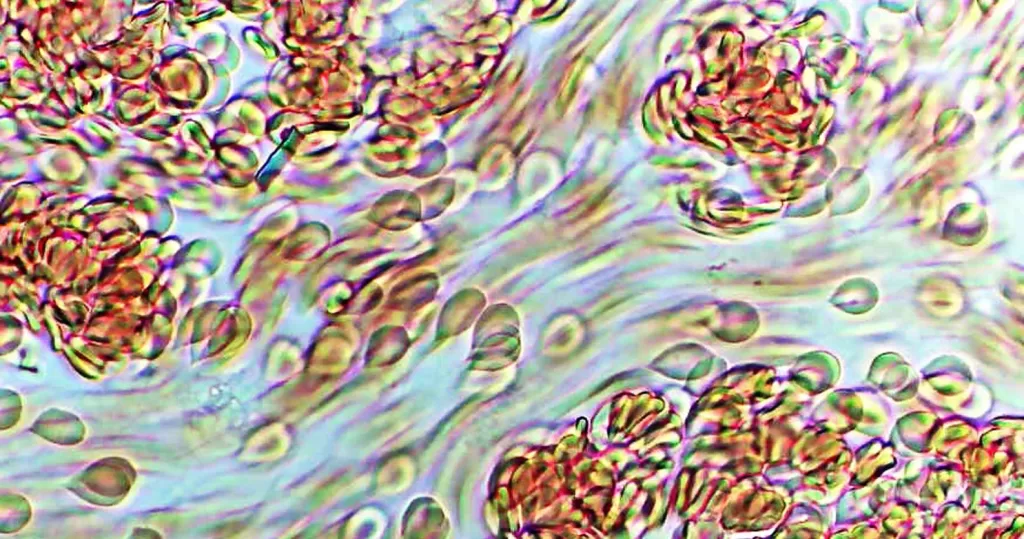
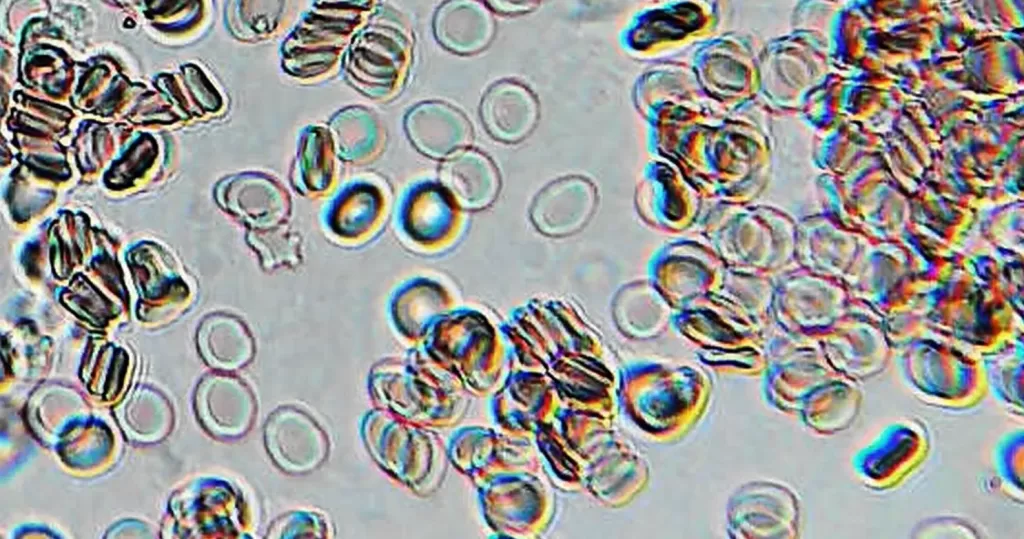
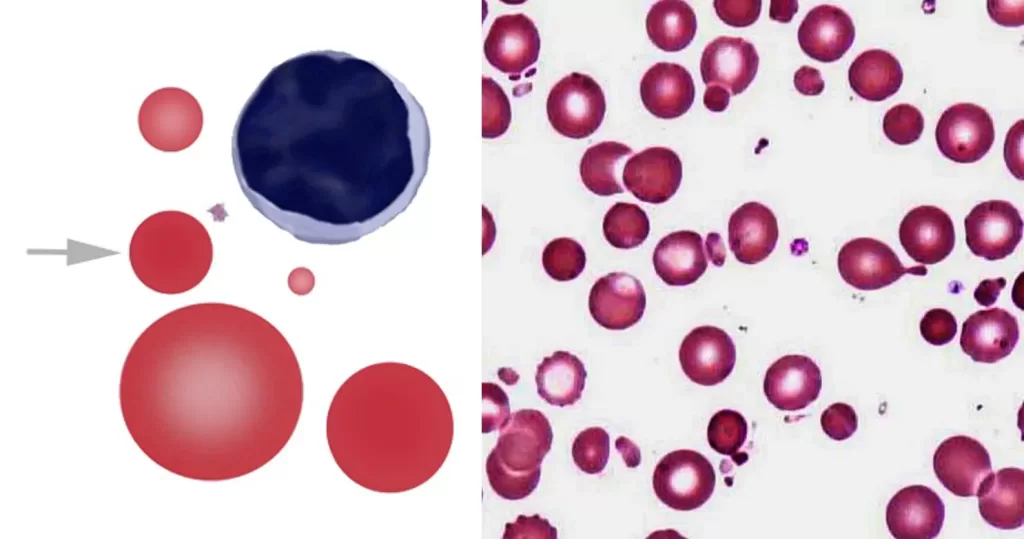
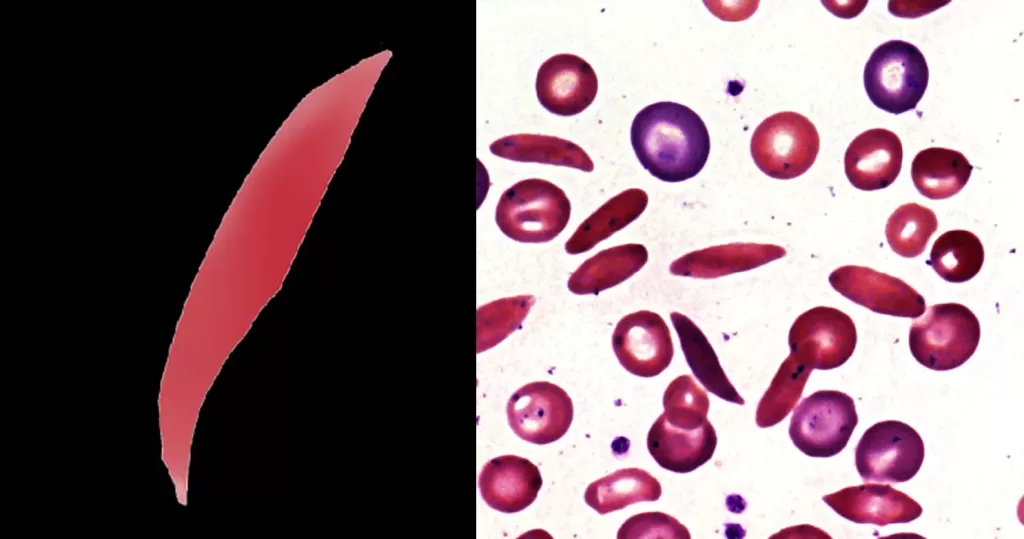
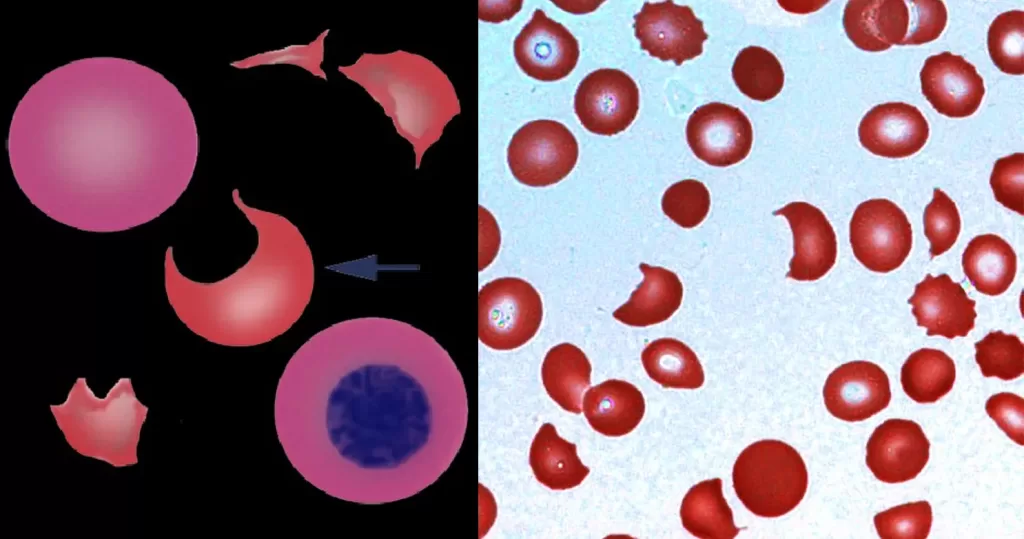
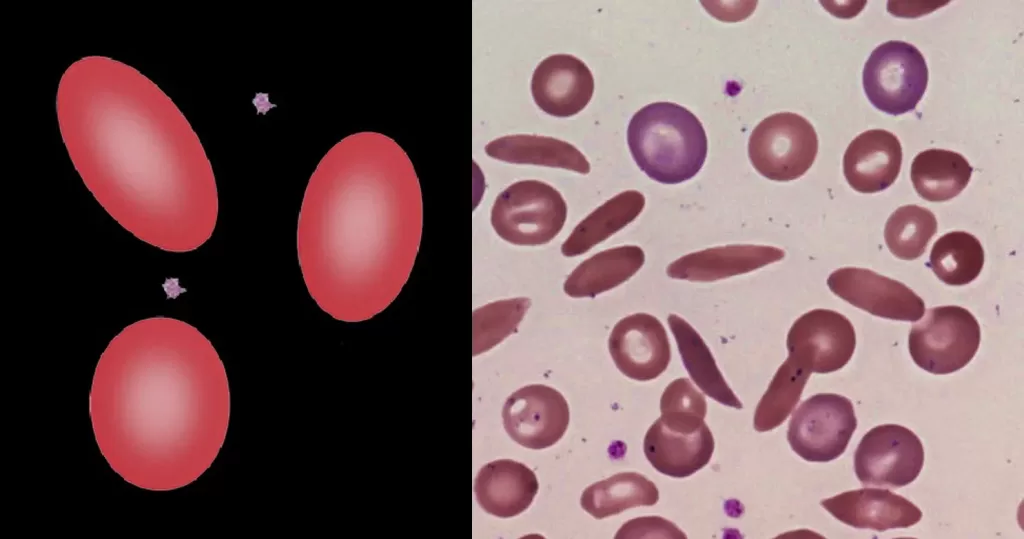
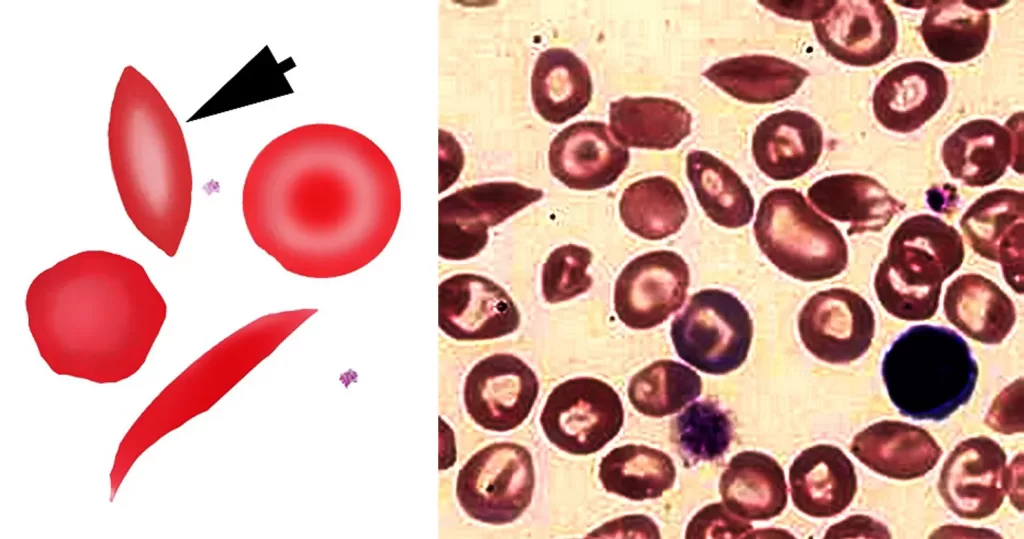
Adjoining monocytes, one more mature than the other. They appear to be suctioning adjoining odd-shaped red cells in order the cleanse them.
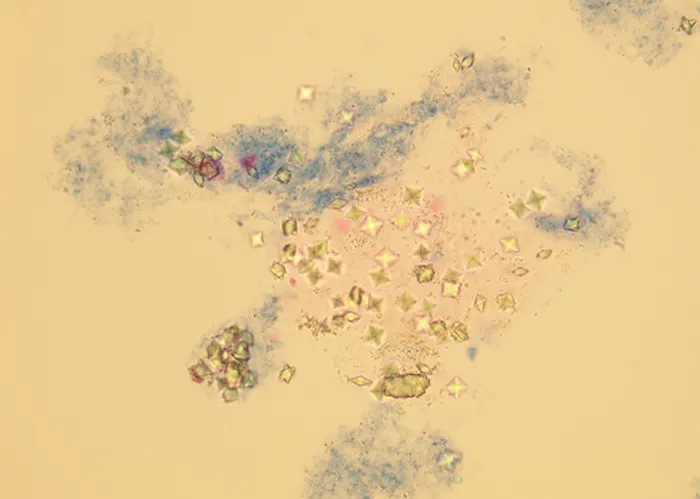
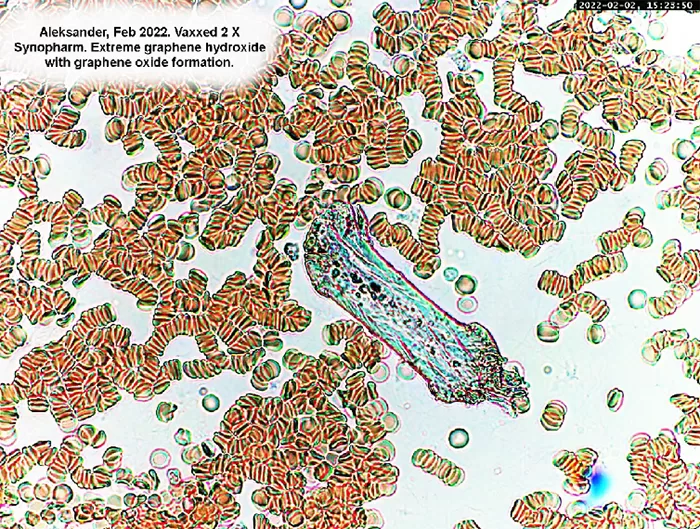
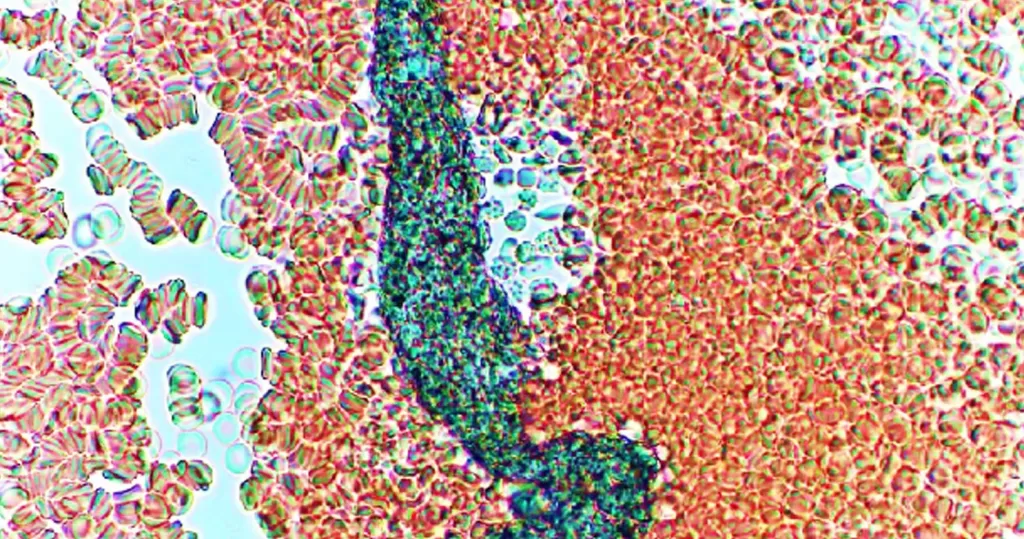
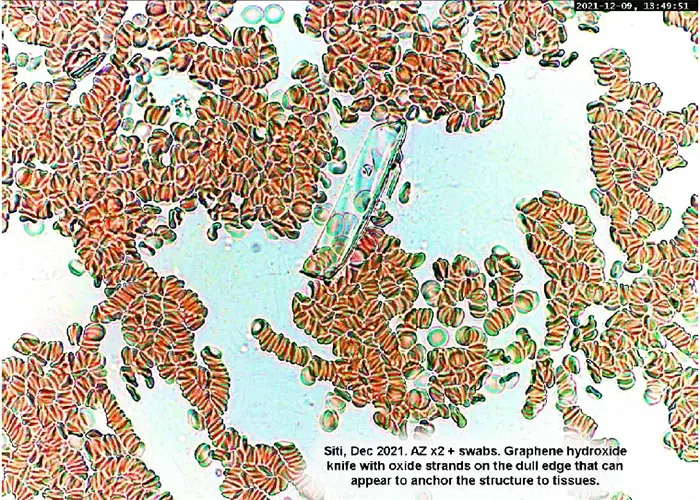
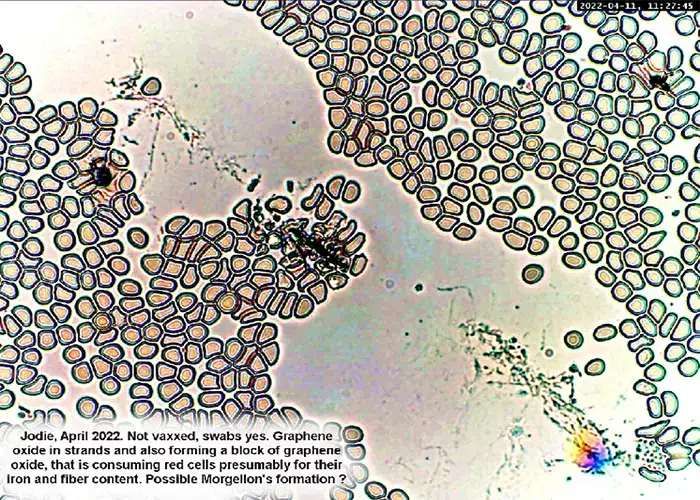
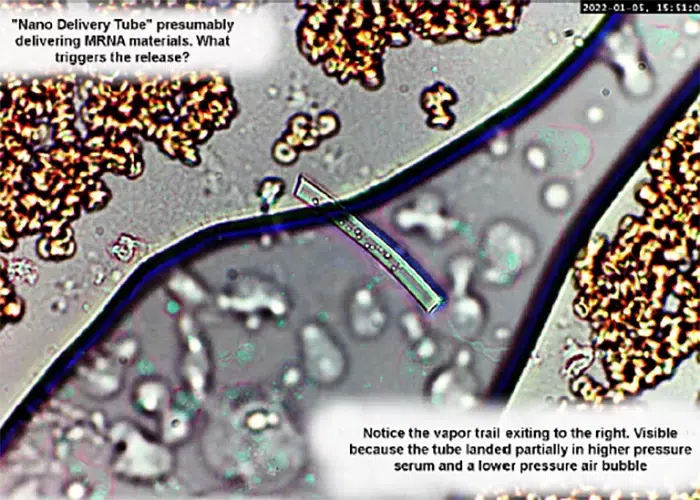
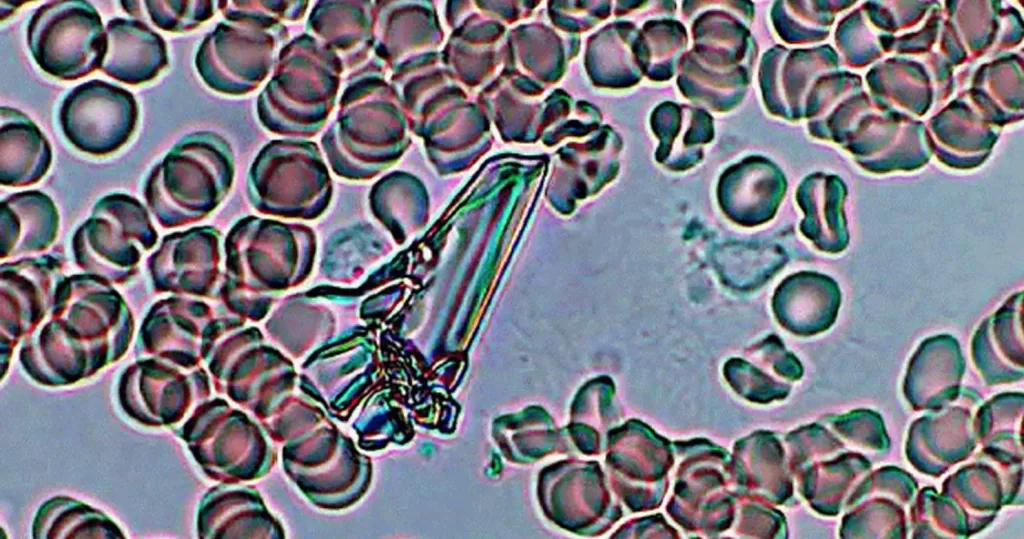
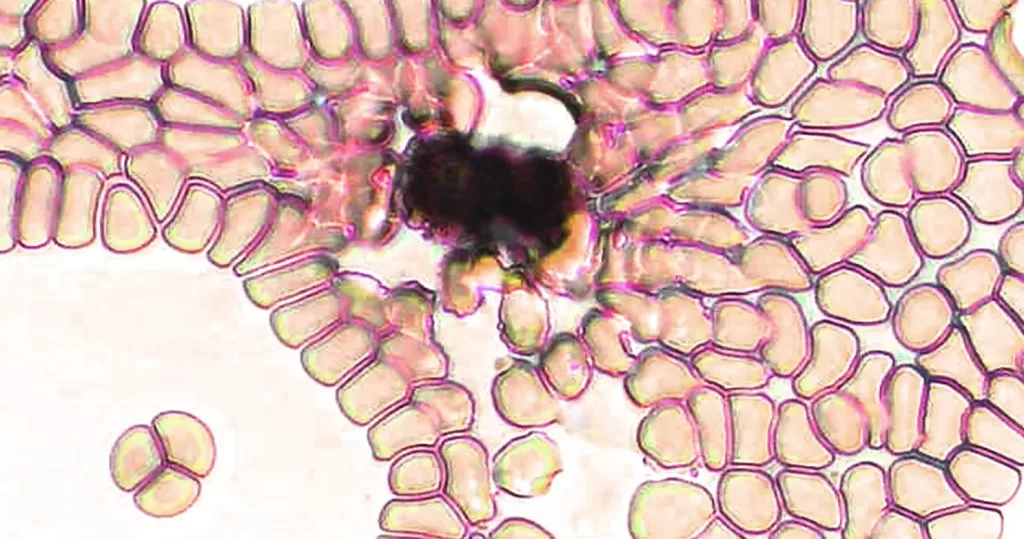
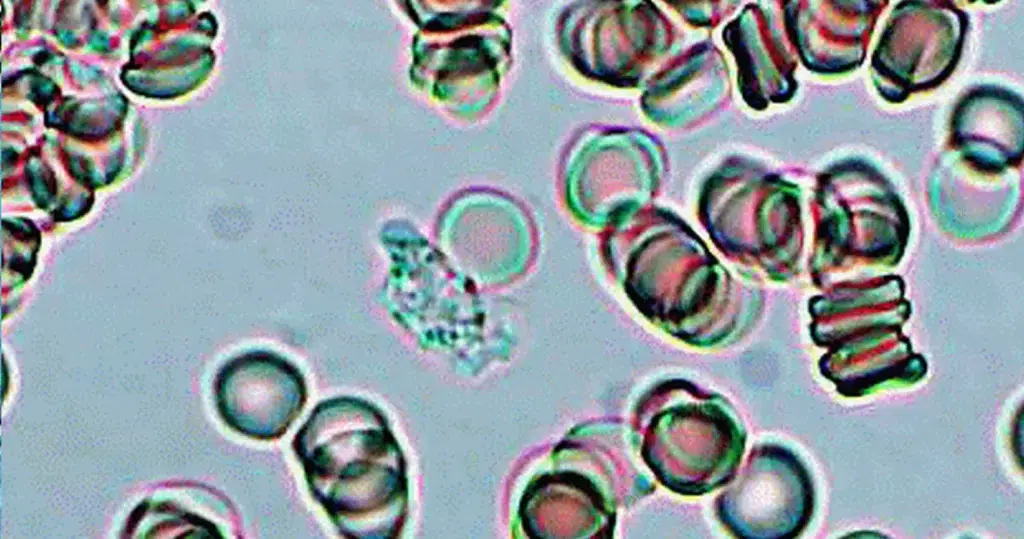
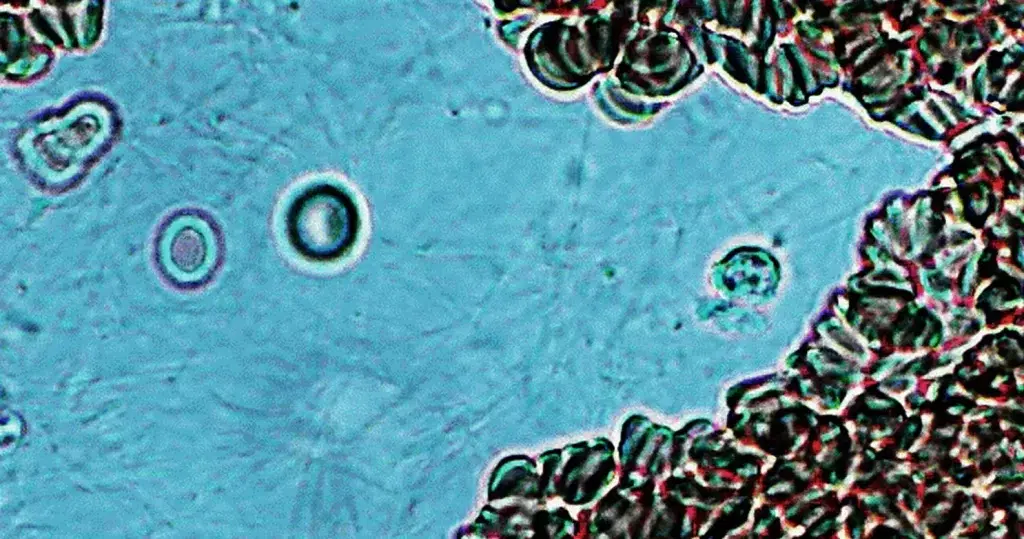
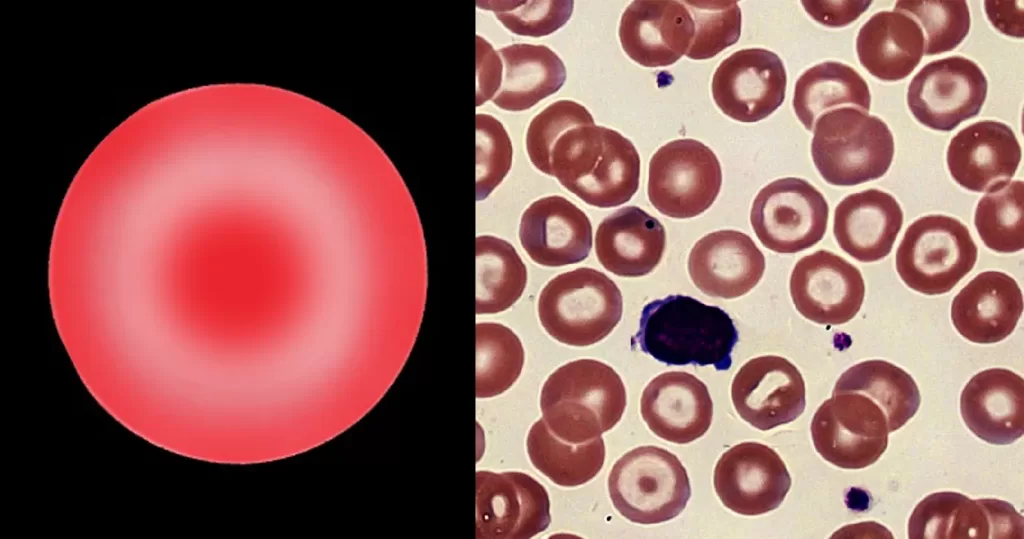
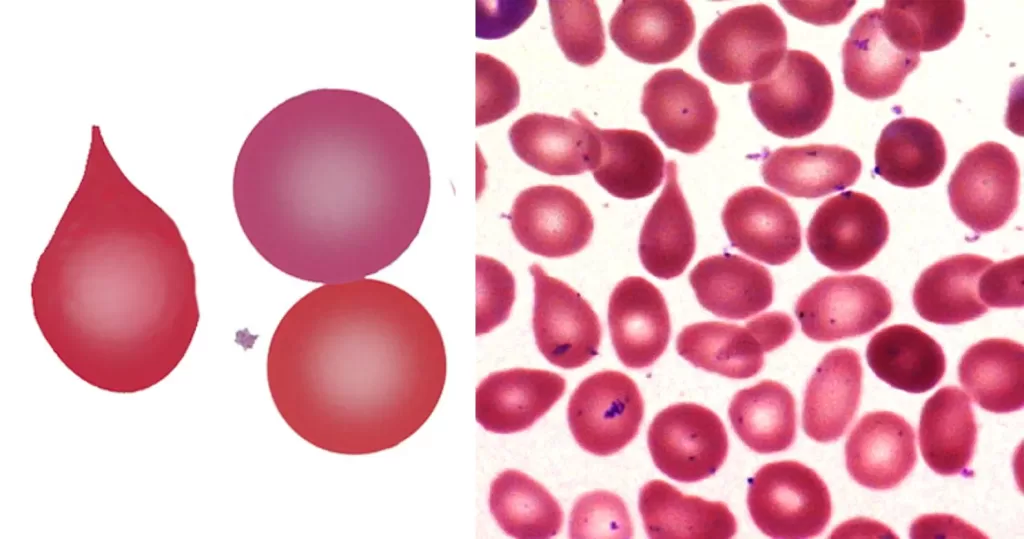
A highly toxic crystal, that appears to leach ferritin or hemoglobin, causing mutation of surrounding red cells.
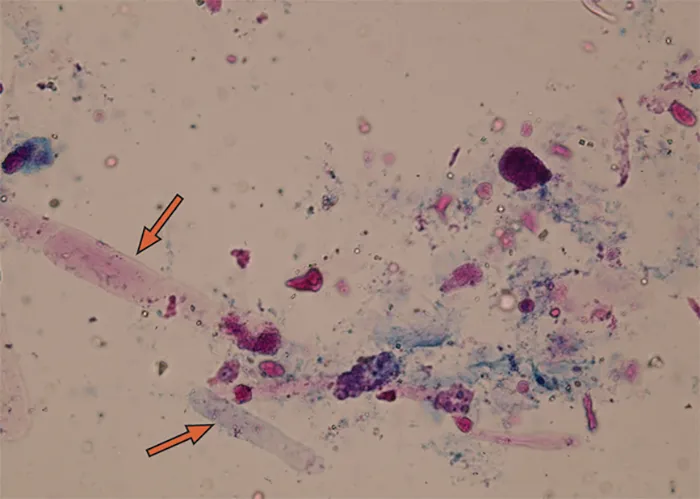
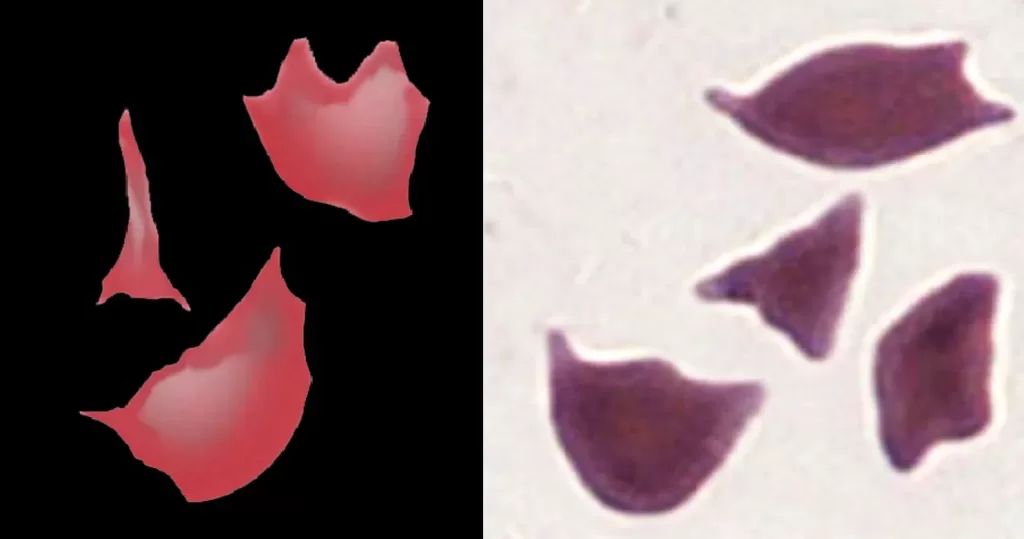
Perhaps 1 monocyte and 2 neutrophils are depleted, exhausted in a futile attempt to neutralize the toxin.
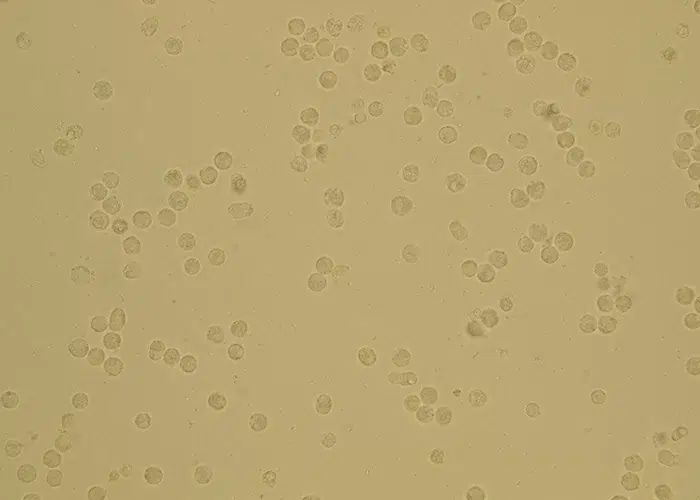
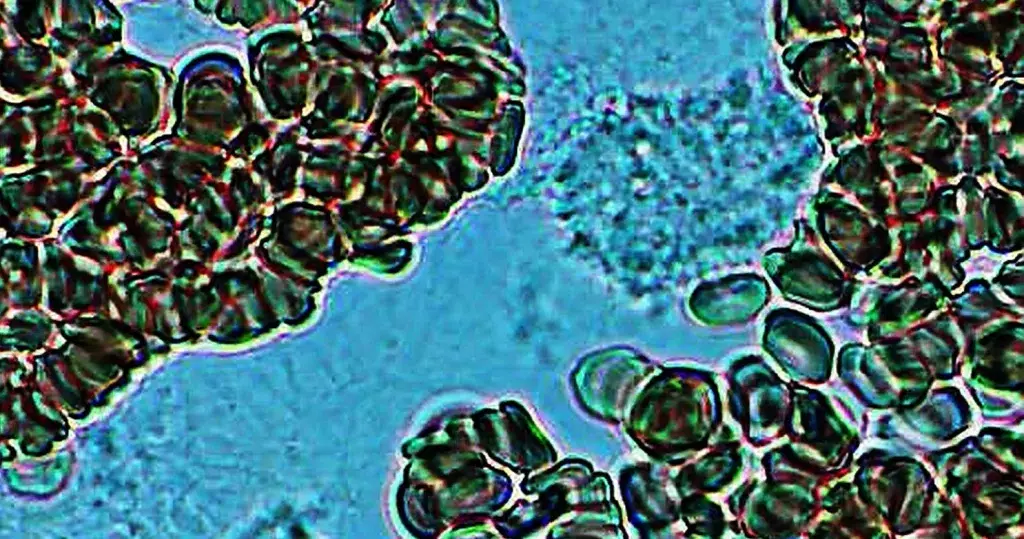
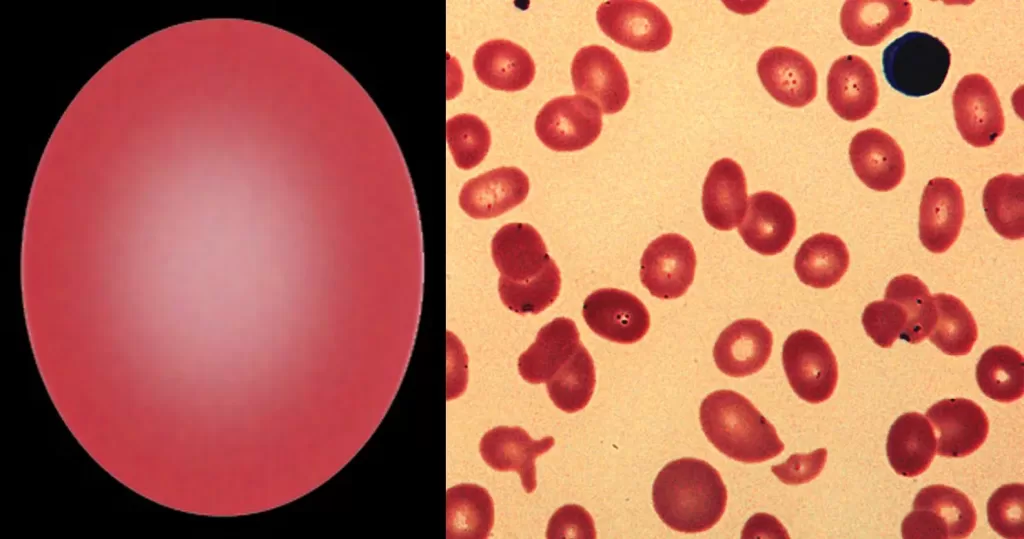
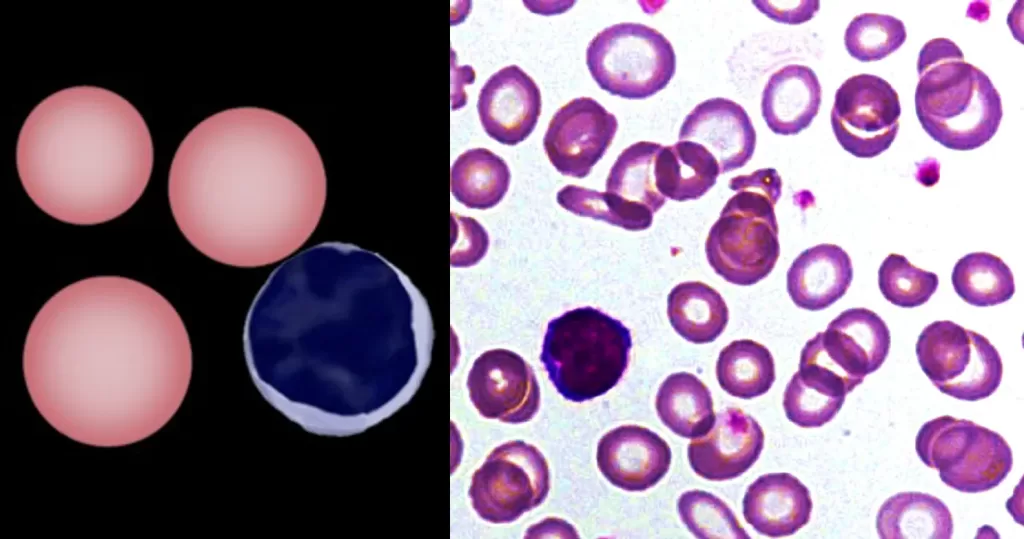
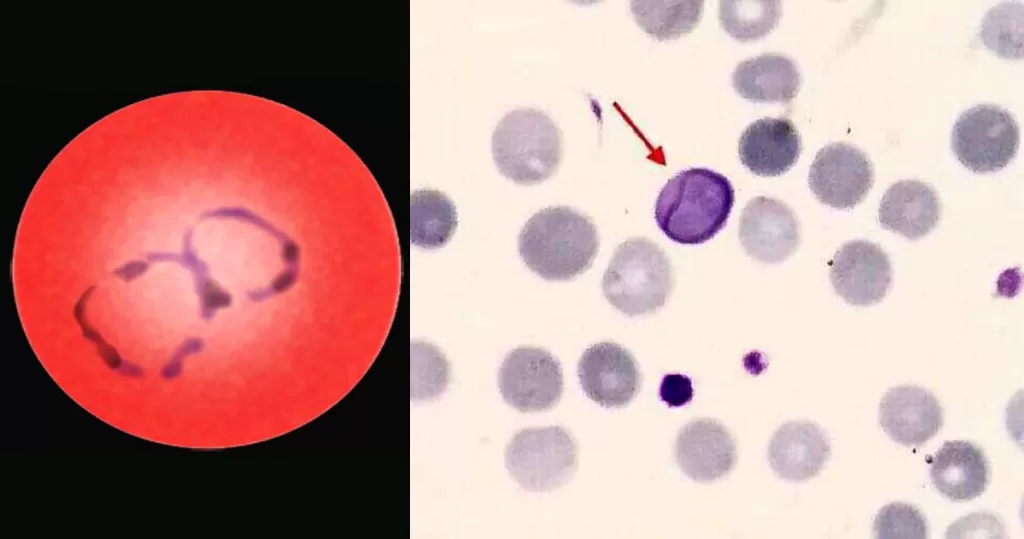
Unstained. 1 large and inactive monocytes (no white dots inside) and possibly 1 inactive lymphocyte (top).